Resources
We have a wide range of resources – from videos to publications – to inspire, inform and help you deliver better places in Scotland.


Shared learning events: Learning Estate Investment Programme
Read about the Learning Estate Investment Programme and how it helps shape great learning environments.

Annual Review 2025
Reflecting on our Past, Present, and Future

Learning locally: co-designing sustainable learning settings
Learning from our pilot project in Armadale West Lothian to test the delivery of the "Learning for Sustainability policy in our places.

Spatial ideas for inclusive and accessible learning environments
Sharing ways design can help create safe and supported spaces to meet the needs of all pupils.

Key principles for inclusive and accessible learning environments
Considerations for creating safe and supported spaces to meet the needs of all pupils

Designing for inclusive and accessible learning environments
How design can help to create safe and supported spaces to meet the needs of all pupils

Design elements for school grounds: ideas to inspire
This resource provides ideas for those seeking to develop their school grounds, and shares creative inspiration for outdoor spaces.

Place skills for plan-making
Helping planning authorities take a place-based collaborative approach to Local Development Plan preparations.

Annual Review 2024
Celebrating a year of collaboration, community-thinking, new perspectives, and design excellence.

PlaceTech Innovation Lab summary report
2024 pilot project summary report

How to embed climate actions in your place
Learning from the Climate Action Towns project

Climate Action Towns Toolkit
A toolkit to support people in towns and communities across Scotland to take place-based climate actions

Annual Review 2023: reflections and projections
A celebration of our work in 2023 and looking forward to 2024.

Pulse project gallery
Our Pulse project gallery includes short examples of various best-practice health development facilities. You can explore our gallery below for various development types ranging from hospitals to dental clinics, its locations, value of the development and the attached SCIM Design Statements.

Pulse image gallery
Our Pulse image gallery includes images of different types of health-based places. In this section of our Pulse gallery, you have access to images of outstanding healthcare facilities that meets the needs of its patients and staff. For more information view our gallery below.

Climate Ready School Grounds
How we can work together to help school grounds in Scotland tackle the climate emergency.
Climate Action Towns: year two review
Reviewing a year of action and ongoing collaboration across the nine towns

Taking action on climate change
Inspiring community-led projects from across Scotland that deliver positive, place-based climate action.

Towards zero carbon places - making it happen at the Place Forum
Key learning points from the Place Forum exploring the role of retrofit and zero carbon buildings to create carbon conscious places.

The power of place in child poverty and cost of living crisis
Find out more about our first Place Forum event and hear about the power of place and collaboration in child poverty and cost of living crisis.
Key Agencies Group Collaborative Local Development Plan Offer
Supporting six planning authorities in taking a place-based collaborative approach to preparing Local Development Plans.

Annual review: reflections and projections
Our work in 2022 and projections for 2023.
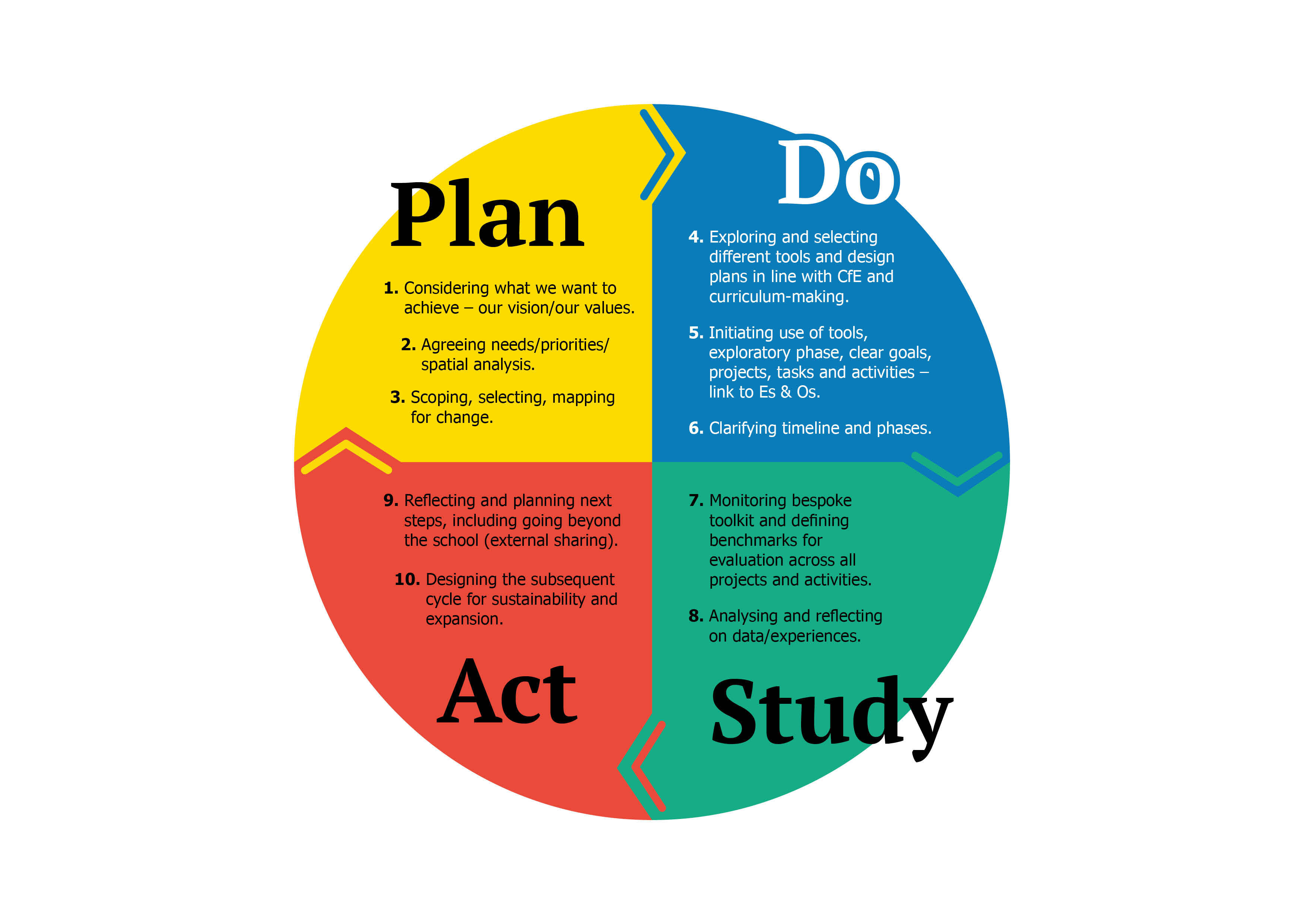
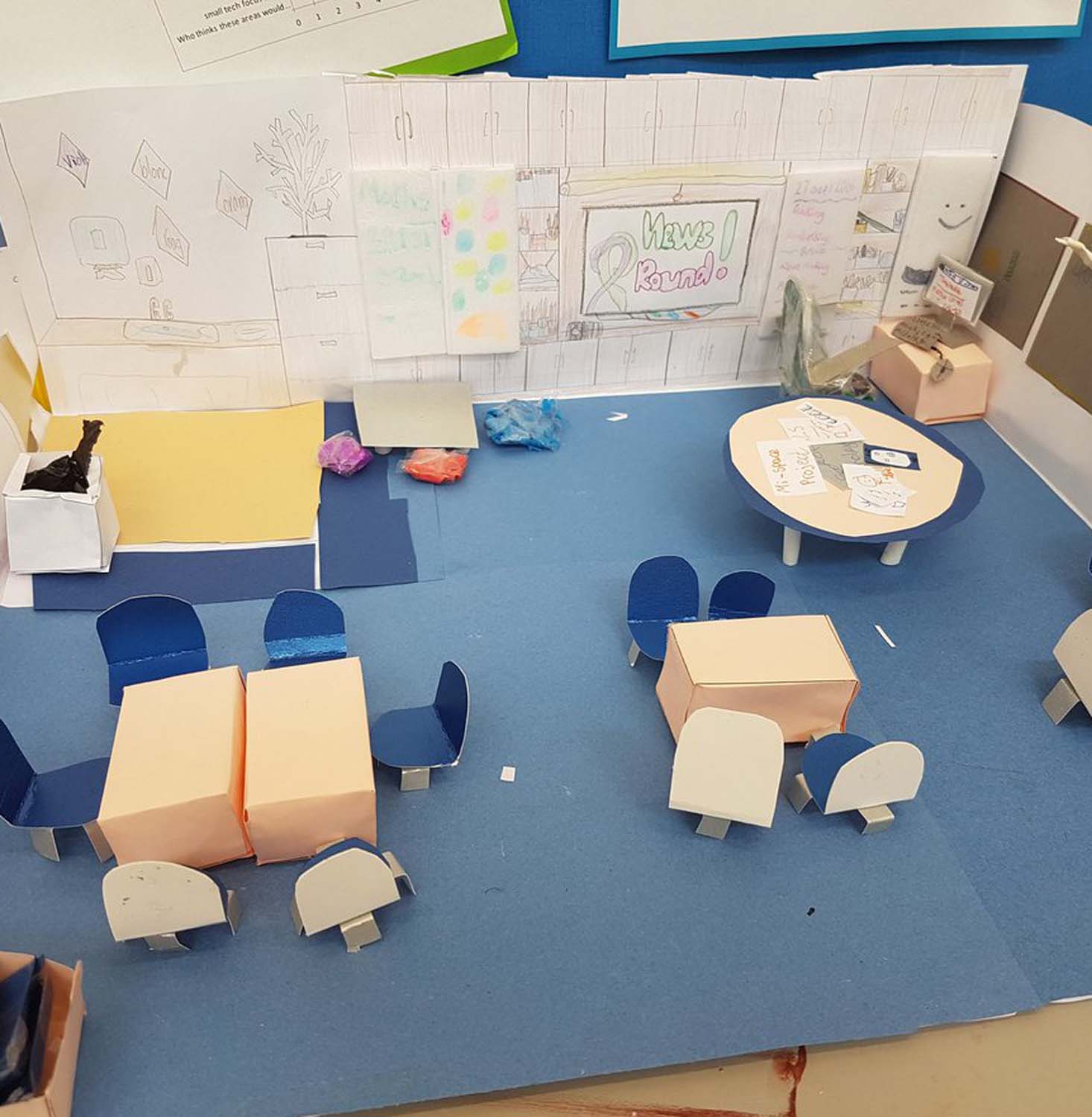
Our Shared Learning Toolkit
Watch the video to find out how the toolkit helps teachers and pupils test ways and design learning spaces.

Climate Action Towns: year one lessons
Key findings and lessons learned from our first year of the Climate Action Towns project.
Place Standard
Working together to improve the quality of places across Scotland.
Scotland + Venice
Learn about Scotland’s participation at the Biennale Architettura over the years.

Public Sector Client Forum: rural futures
Catch up on our rural futures Public Sector Client Forum and hear from organisations helping to create thriving countryside communities.

Planning performance framework report 2019-20
This report highlights how we supported the delivery of better outcomes through the planning system in 2019-20.

Housing to prioritise people
We support the development of homes that are designed to strengthen communities.

Climate Action Towns
We worked with local communities to support place-based climate action in a network of small Scottish towns.
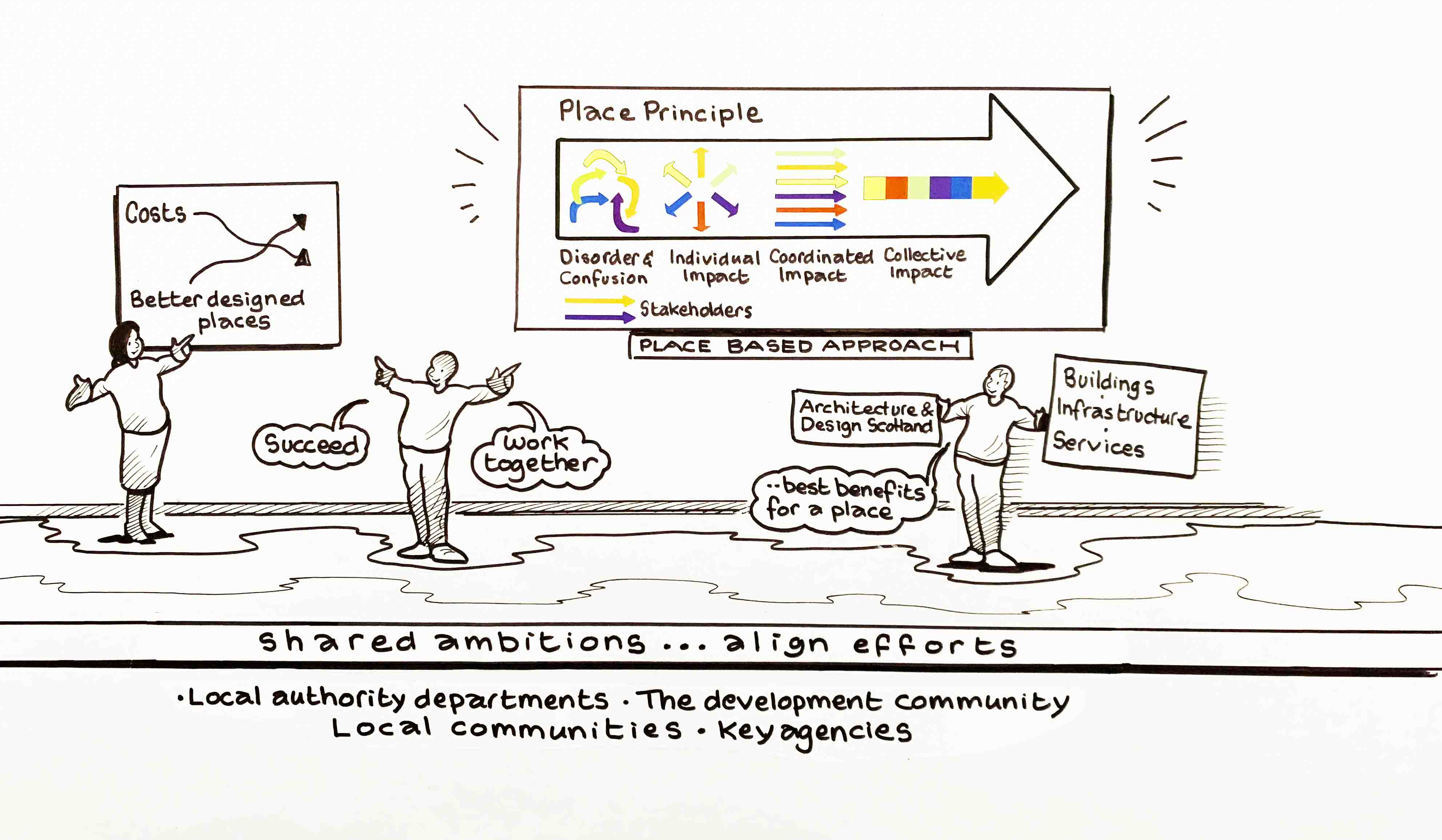
The eight principles of a carbon conscious place
The eight principles of a carbon conscious place support a holistic approach to designing and adapting places to reduce, repurpose and absorb carbon.

LAUDF 15: Designing for net zero – event report
Explore all the learning from our first online Local Authority Urban Design Forum event on 1 March 2022.
Furniture, fixtures and equipment: toolkit and tips
Use our practical guide for furnishing and equipping spaces and settings to deliver better learning environments.

Health design advice
Working collaboratively to design health and social care facilities for patients, staff and communities.

Connecting people, places and learning
Working collaboratively to design learning estates for Scotland's new generation of learners.

Town centre living
By working together we can re-imagine our town centres to create caring places for all.

Designing for a changing climate: carbon conscious places
We are working closely with communities and local authorities across Scotland who are designing carbon conscious places.

Alva Pathfinder toolkit
An introduction to the approach we took and tools we used during the Alva Pathfinder work.
Alva Pathfinder: application of the Place Standard tool
Find out how the Place Standard tool was used as part of the Alva Pathfinder project.
2021 Annual Review: a reflection of our work
Our 2021 Annual Review highlights areas of work and shares some of your feedback. Our staff also reflect on their highlights of the year.

Exploring flood risk management for Kilmarnock
The sharing of good practices in blue-green infrastructure.

Planning performance framework report 2020-21
This report highlights how we supported the delivery of better outcomes through the planning system in 2020-21.

Andy MacMillan Memorial Lecture 2021 – Dr Jos Boys
A lecture recording from Dr Jos Boys.
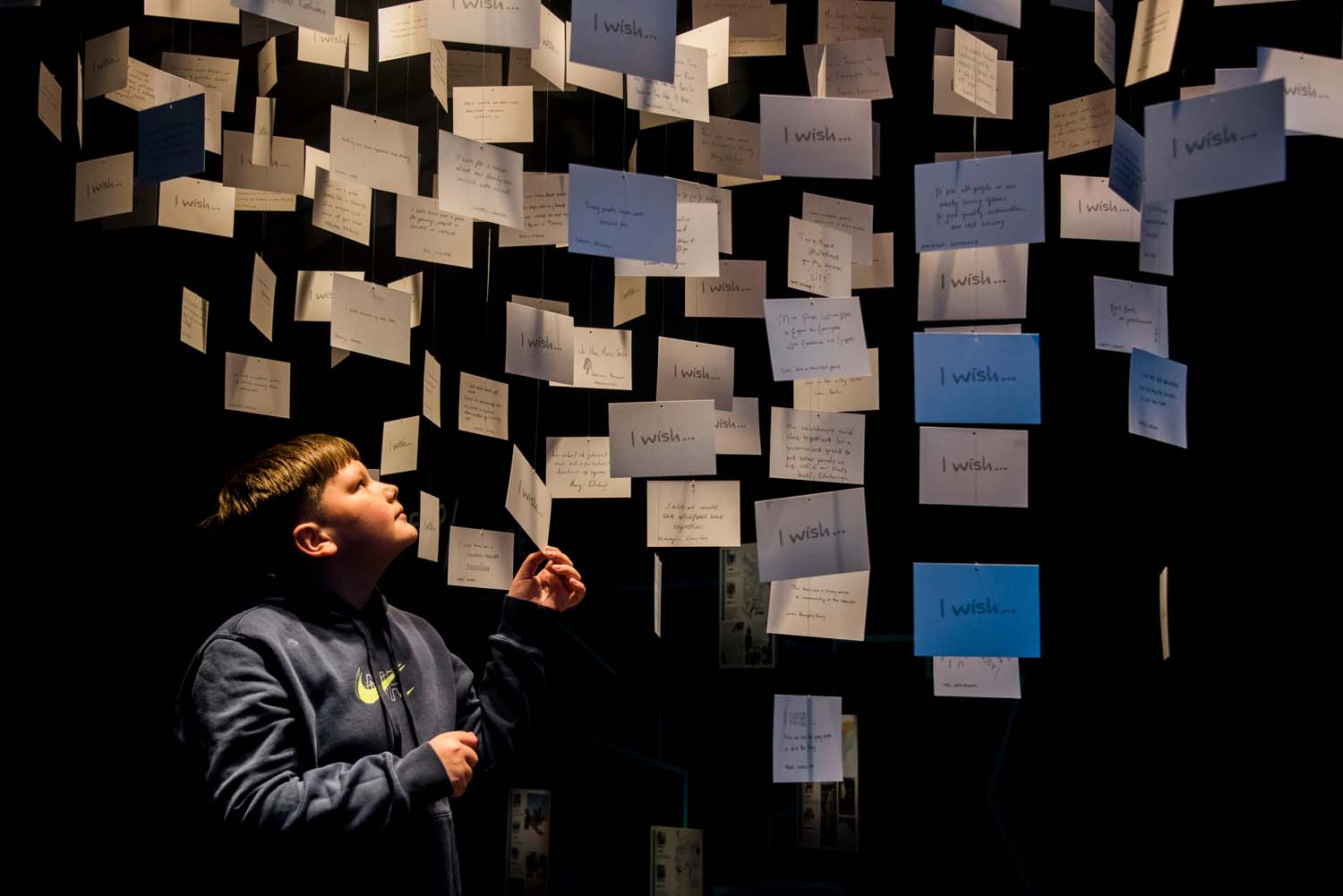
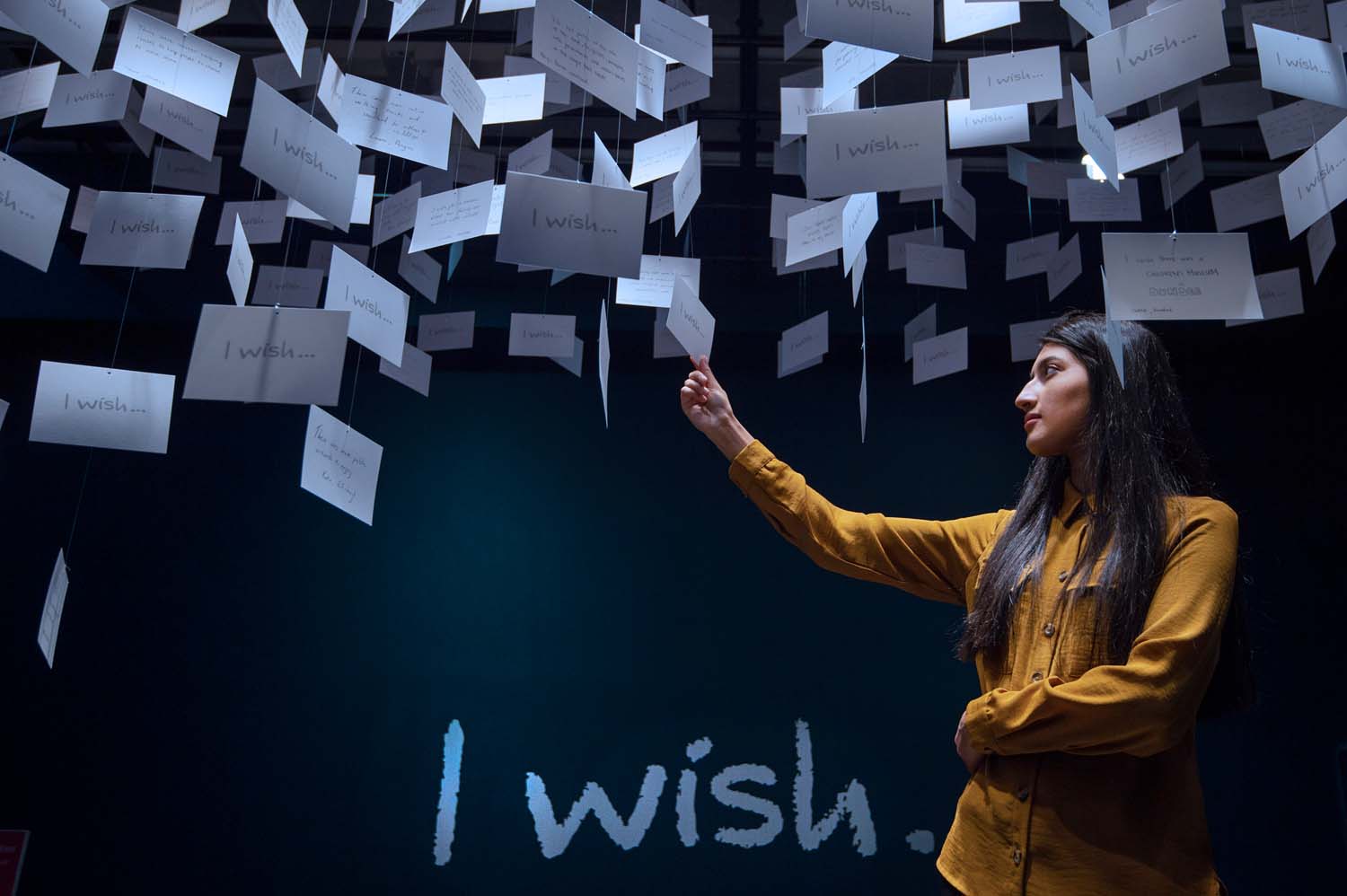
What if…?/Scotland opening event: launch and Q&A recording
Shared hopes, dreams and wishes for the future of the places where we live.
Corporate Plan 2021-24
Our Corporate Plan 2021-24 sets out how we will deliver the first stage of our Corporate Strategy 2021-31.

Corporate Strategy 2021-31
Our corporate strategy sets out how we will make the Place Principle an everyday reality in the way Scotland’s places are created, adapted and sustained.

Annual Review 2020: our year in review
Despite the challenges of lockdown and the closure of our offices, we have continued to deliver high quality and important work.
Why take a place-based approach to housing?
A short video introducing our skills document supporting a place-based approach to housing.
Report: designing for a changing climate
Explore what we learned from the first year of our work into designing for a changing climate.
Scotland +Venice: Fellowship Programme 2018
Five students had the opportunity to take part in Scotland’s critically acclaimed response to the Biennale Architettura 2018. Here you can read their work.

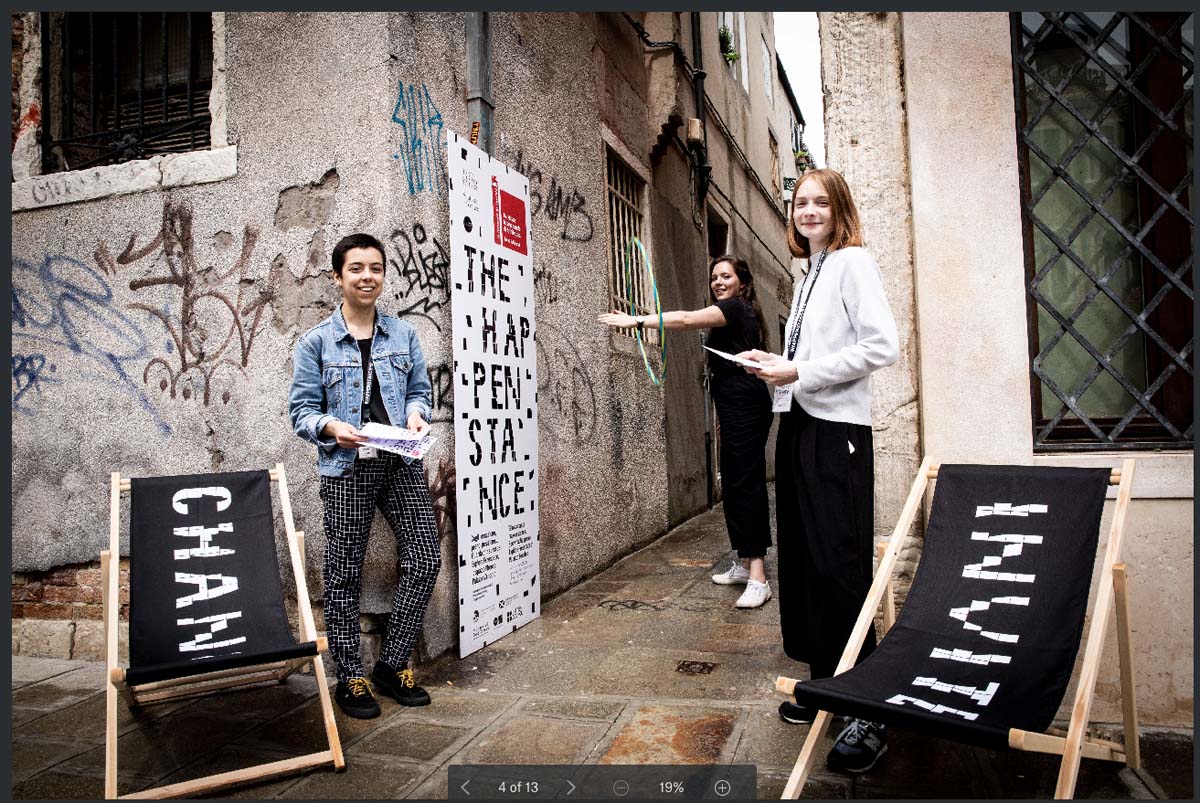
The Happenstance: Cultural Connectors Forum programme
The handout for the Cultural Connectors Forum, which took place in Venice in November 2018.
The Happenstance: translations of Taiwanese articles
The translations of three articles about The Happenstance by Taiwanese journalist Sharon Ma.

The Happenstance: the story of an airborne gondola
A first-hand account of a film screening at The Happenstance about an airborne gondola.
Scotland + Venice: The Happenstance dispatches
A series of 12 publications or ‘dispatches’ exploring the themes and learning from The Happenstance.

Andy MacMillan Memorial Lecture 2020 – Jude Barber, Collective Architecture
A video of the Andy MacMillan Lecture delivered by Jude Barber in 2020.

Engaging communities during lockdown
Lessons from practitioners

PSCF2020: Ben Twist and Jim MacDonald discussion
A series of interviews for the Public Sector Client Forum 2020 event.

PSCF2020: world cafe sessions
A series of short videos from the Public Sector Client Forum 2020 event: designing for a changing climate.
PSCF2020: designing for a changing climate
A selection of online resources from the Public Sector Client Forum event 'Climate, health and place' including presentations, interviews and more.

Local authority urban design forum 14 - newsletter - January 2020
A newsletter on approaches to market-led housing

Housing to 2040
Explore how we supported the Scottish Government’s Housing to 2040 consultation with our series of workshop reports, interviews, and an exhibition.
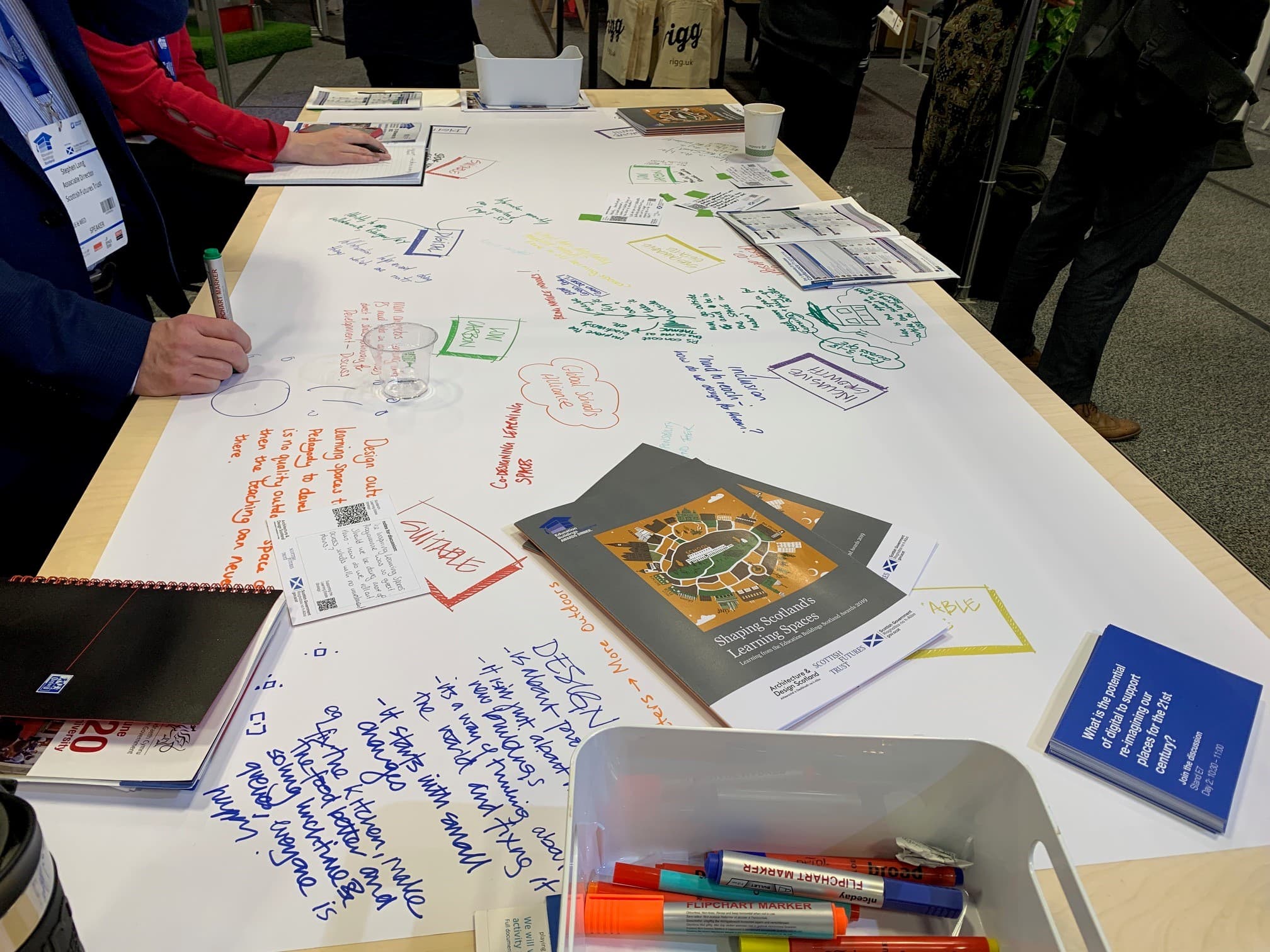
Shaping Scotland’s learning spaces
Reflecting on award-winning projects from the Education Buildings Scotland Awards.

Planning performance framework report 2018-19
This report highlights how we supported the delivery of better outcomes through the planning system in 2018-19.

Place Standard videos from Making Place Conference 2019
Interviews of the attendees at the Making Place Conference.
Local authority urban design forum 13 - newsletter - May 2019
A newsletter on approaches to active travel

Town centre living: ten principles of a caring place
Explore how town centres can be adapted to support us as we get older and what a caring place could look like.
Local authority urban design forum 12 - newsletter - December 2018
A newsletter on approaches to placemaking, design review and assessment

Inspiring Learning Spaces Toolkit
Explore how to get the best from your learning environments with a clear process and exercises designed to help you manage change effectively.

Planning performance framework report 2017-18
A report on how we supported the planning system in 2017-18.
Local authority urban design forum 11 - newsletter - June 2018
A newsletter on housing delivery: from masterplans to plot passports

Inspiring Learning Spaces
Learn how the conventional classroom is being reimagined, with learners at the heart of the process, into a space that boosts learners’ confidence and engagement.

Guide to the NHSScotland Design Assessment Process (NDAP)
An introduction to the NHS Scotland Design Assessment Process (NDAP) and how we at Architecture and Design Scotland can help.

What is an SCIM Design Statement?
An introduction to the Scottish Capital Investment Manual (SCIM) Design Statement.

Outdoor learning: the extended classroom
A publication on the benefits of outdoor learning for your school environments.

Town centre living: Place Challenge 2015
Creating town centres as living places that re-use existing spaces to deliver housing, employment, and services.

Stalled Spaces Scotland
Featuring a comprehensive guide and real-life examples of success stories from Stalled Spaces Scotland projects.

Quality and efficiency - A primary care reference study
This resource aims to share lessons from a reference design project looking at primary care.
Graphical communication in plan-making
This resource outlines the benefits of and practical approach to using graphics when communicating plans.

A guide to participation: what we have learnt so far
Find out how you can get a variety of school users to participate in designing your schools.
Local authority urban design forum 03 - workshop report - May 2014
A workshop session on how different places in Scotland are approaching the development planning process
Local authority urban design forum 02 - newsletter - November 2013
A newsletter on sharing experience on design quality through planning guidance

Reference guide: commissioning healthcare developments
A brief guide for stakeholders, project board and steering group members taking part in a healthcare building development.

The natural health service
A green vision for NHS Scotland’s outdoor estate.
Search yielded no results